








Healthcare cybersecurity in 2026 is defined less by novel attack techniques than by a widening gap between which controls organizations report having and which controls are reducing loss.
Our portfolio data from 2023 through mid-2025 shows that social engineering, backup gaps, and weak data governance drive the majority of material losses in healthcare claims.
Director of Customer Engagement at Resilience.
The headline numbers already tell part of the story. U.S. healthcare organizations reported 275 million records breached in 2024, more than double the prior year and the largest single-year exposure in the sector’s history.
Ransomware attacks against healthcare climbed 32 percent over the same period, and the Change Healthcare incident alone exposed an estimated 190 million individuals.
The useful question for CISOs, CFOs, and boards is not how big the breaches got. It is what claims data reveals about which threats are driving losses and which investments are measurably reducing them.
What is driving healthcare cyber losses right now
Social engineering drove 88 percent of material losses across our portfolio in the first half of 2025, and healthcare-specific claims followed the same pattern. Phishing, business email compromise, and vendor compromise show up repeatedly in the underlying incident data, alongside backup gaps that leave organizations exposed when ransomware lands and tracking pixel errors that quietly expose patient information.
The threat actor landscape is also more distributed than the most visible groups suggest. While BlackCat and Cl0p appeared most frequently in healthcare-related activity, the actual successful intrusions were spread more evenly across operators like Interlock, Lockbit, and Medusa. That distribution matters for defenders, hardening against the loudest names while remaining exposed to lesser-known operators is a specific failure mode the data keeps surfacing.
Extortion demands have also climbed. In the first half of 2025, healthcare-related incidents in the portfolio carried extortion demands as high as $4 million. Those costs carry a different weight when patient care is at stake and the alternative to paying is not just operational disruption but clinical risk.
Which cybersecurity controls reduce risk in healthcare
Five controls show the highest measurable risk reduction in healthcare environments in our portfolio: secure email gateways, immutable backups, multi-factor authentication on all remote access, formal data governance, and regular tabletop exercises that include clinical operations. None of these are exotic, and most healthcare organizations can implement them without a transformational budget request.
Two findings in the portfolio data stand out as specific to healthcare. Immutable backups deliver stronger risk reduction in healthcare than in other industries on average, largely because ransomware against clinical systems creates a different recovery calculus than ransomware against, say, a manufacturer’s ERP software. And organizations with a formal data governance committee see more than three times the risk reduction compared to peers in other sectors, a reflection of how much of healthcare’s exposure lives in the data layer itself, not just the endpoint.
The pattern matters more than any single control. Every control on the list operates before or during an incident, not after. That is where the measurable risk reduction lives.
Why the budget conversation keeps breaking down
Healthcare CISOs face a specific version of a universal problem: the controls with the highest modelled risk reduction are often the least visible to executive leadership, and the controls most visible to executive leadership are often the ones with the weakest loss-reduction signal. That asymmetry is what quantifying cyber risk is meant to close.
In practice, the healthcare organizations getting ahead on this are doing three things. They are translating control adoption into dollar terms their CFO can evaluate against other capital decisions. They are prioritizing spend against the specific controls the claims data identifies as high-ROI in their sector, rather than defaulting to a framework checklist. And they are running tabletop exercises that include clinical leadership, not just IT, because the decisions that determine whether a ransomware event becomes a patient-care event are not purely technical.
What this looks like in practice
Two contrasting examples from our portfolio make the point. A mid-sized regional health system believed its security posture was stronger than it turned out to be and discovered the gap the hard way during a major ransomware incident, including the discovery that clinical imaging files had been left out of its backup strategy. Recovery costs, regulatory exposure, and care disruption compounded.
A mid-market biotechnology firm took a different path. It built a quantified, prioritized cyber risk program, mapped its controls against its largest modelled loss scenarios, and was able to redirect security spending toward the controls with the highest return. When an attempted business email compromise hit, the controls worked, and the claim never materialized.
The gap between those two outcomes was not budget. It was how each organisation decided what to spend the budget on.
What healthcare security leaders should do now
Three moves are defensible, specific, and available without a transformational program. First, audit the organization’s backup posture against a realistic ransomware scenario, including clinical systems and imaging data, not just administrative files. In our portfolio, backup gaps are one of the single largest drivers of healthcare ransomware severity.
Second, measure social engineering resilience directly. Tabletop exercises, phishing simulations, and control reviews of email gateway posture are faster to run than most organizations assume, and social engineering’s share of material loss makes them high-ROI by any reasonable measure.
Third, translate the top three or four risk scenarios into dollar terms and walk them to the board. The CFO conversation goes differently when the ask is framed as loss reduction, not technology spend. Risk quantification is what makes that reframe defensible.
This shows the need for risk quantification on plausible material loss scenarios; without it, budget conversations stay abstract while the exposure stays real. It requires a willingness to let the claims data, rather than the vendor roadmap, set the priority list.
We feature the best cloud backup services.
This article was produced as part of TechRadar Pro Perspectives, our channel to feature the best and brightest minds in the technology industry today.
The views expressed here are those of the author and are not necessarily those of TechRadarPro or Future plc. If you are interested in contributing find out more here: https://www.techradar.com/pro/perspectives-how-to-submit














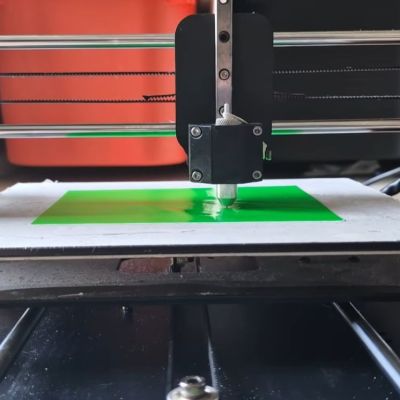 Replacing a 3D printer’s extruder with a cutting blade seems like an easy way to do things like vinyl cutting, but you cannot just put on any blade and expect good results. The right type of blade is called a drag knife and it’s designed so that it follows the direction in which you’re cutting. You can get these in dedicated vinyl cutting machines, as well as in the form of attachments for the likes of CNC machines. How to use them with an old Anycubic Mega S FDM printer is demonstrated
Replacing a 3D printer’s extruder with a cutting blade seems like an easy way to do things like vinyl cutting, but you cannot just put on any blade and expect good results. The right type of blade is called a drag knife and it’s designed so that it follows the direction in which you’re cutting. You can get these in dedicated vinyl cutting machines, as well as in the form of attachments for the likes of CNC machines. How to use them with an old Anycubic Mega S FDM printer is demonstrated 





































You must be logged in to post a comment Login